

Photo by Geo Days on Unsplash
CURRENT CONCEPTS IN CLEANING AND SHAPING OF ROOT CANAL SYSTEM
INTRODUCTION
Endodontic therapy involves treating vital and necrotic dental pulps so that patients can retain their natural teeth in function and aesthetics.
Endodontic treatment mainly consists of three steps:
- Cleaning and shaping of the root canal system
- Disinfection
- Obturation
Although successful therapy depends on many factors, one of the most important steps in any root canal treatment is canal preparation.
This is essential because preparation determines the efficacy of all subsequent procedures and includes mechanical debridement, creation of space for medicament delivery, and optimized canal geometries for adequate obturation.
Although endodontic instruments can shape a root canal, irrigants play an important role in cleaning the root canal system.
The aim of cleaning is the removal of tissue remnants and bacterial biofilms in order to allow close adaptation of the root filling to the canal walls.
DEFINITIONS
- Cleaning: It comprises the removal of all potentially pathogenic contents from the root canal system.
- Shaping: The establishment of a specifically shaped cavity which performs the dual role of three-dimensional progressive access into the canal and creating an apical preparation which will permit the final obturation instruments and materials to fit easily.
MECHANICAL OBJECTIVES
- Should have a continuous, tapering, conical shape, with the narrowest cross-sectional diameter apically and the widest diameter coronally.
- The walls should taper evenly toward the apex and should be confluent with the access cavity.
- To give the prepared root canal the “quality of flow,” i.e., a shape that permits plasticized gutta-percha to flow against the walls without impedance.
- Should keep the apical foramen as small as practical.
- Should shape and clean the canal without transporting the apical foramen.
BIOLOGICAL OBJECTIVES
There were also four important biological objectives that are as follows:
- Procedures should be confined to the roots themselves.
- Necrotic debris should not be forced beyond the foramina.
- All tissues should be removed from the root canal space.
- Sufficient space for intracanal medicaments and irrigation should be created
CLINICAL OBJECTIVES
- The clinician should evaluate the tooth to be treated to ensure that the particular tooth has favorable prognosis.
- Before performing cleaning and shaping, the straight line access to canal orifice should be obtained.
- All the overlying dentin should be removed and there should be flared and smooth internal walls to provide straight-line access to root canals
INSTRUMENTS USED FOR PREPARATION
Classification of Endodontic Shaping Instruments:
- Group I: Hand-operated endodontic instruments
- Barbed broaches and rasps
- K-type reamers and files
- Hedstroem files
- Group II: Low-speed stainless steel endodontic instruments with latch-type attachments
- Gates-Glidden drills
- Peeso reamers
- Group III: Ultrasonic and sonic instruments
- Group IV: Engine-driven nickel–titanium endodontic instruments (most commonly used)
- Rotary instrumentation
- Reciprocating instrumentation
- Canal adaptive instrumentation
1. Self-adjusting file (SAF)
- XP-Endo Shaper and Finisher
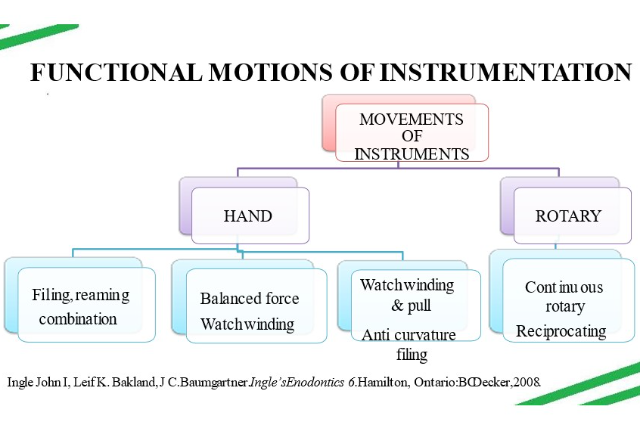
REAMING
- Clockwise rotating pushing motion. (quarter to half turn)
FILING MOTION
- Push-pull motion
COMBINATION OF REAMING & FILING
- Quarter turn clockwise pushing motion (reaming)+ subsequent withdrawal(filing).
Watch winding
- Back & forth reciprocation in clockwise – counter clockwise motion.
- Angle of rotation(30°- 60°)
- K-type instrument
Watch winding & pull
- Additional pull stroke
- H files
BALANCED FORCE
- Clockwise with a quarter turn
- Counter clock wise + push
- Clockwise + pull
Not with H files & broaches
ANTICURVATURE FILING
- Abou Rass,Frank,Glick
- Prevent perforation in furcal areas
- Filing away from the inner curve of root
BASIC PRINCIPLES OF CANAL INSTRUMENTATION
- Straight line access to the canal orifices.
- Files are always worked with in a canal filled with irrigant.
- Retaining its original form and the shape.
- Explore the orifice with smaller file to gauge the canal size and configuration.
- Use instruments in the sequential order without skipping sizes.
- Instruments should be kept in confines of the root canal to avoid any procedural accidents.
- Instrument binding on insertion should be avoided.
- After each insertion and removal of the file, its flutes should be cleaned and inspected.
- Smaller number instruments should be used extravagantly.
- Regular recapitulation is done.
- Over preparation and too aggressive over enlargement of the curved canals should be avoided
- Large apical foramen –apical stop not possible.
- Overusing of larger files should be avoided.
- Never force the instrument in the canal.
- Establish the apical patency before starting the biomechanical preparation of tooth.
GUIDELINES FOR SHAPING OF ROOT CANAL
- The tooth to undergo root canal therapy is identified.
- The rubber dam is applied and the field of operation is disinfected by scrubbing with a sterile cotton-tip applicator saturated with a 5.2% solution of sodium hypochlorite.
- In posterior teeth, after complete removal of the roof of the pulp chamber, the coronal pulp is removed with sharp endodontic spoon excavators.
- The chamber is irrigated with a 5.2% solution of sodium hypochlorite and is dried with suction.
- Next, the canal orifices are located by probing with endodontic explorers along the anatomical grooves located in the chamber floor and leading to the root canals or at the point angle formed by the walls and floor of the pulp chamber.
- These anatomical grooves, sometimes called the dentinal map, unite the canal orifices that are present at the end of the grooves.
- The grooves are darker than the floor of the pulp chamber.
TECHNIQUES OF ROOT CANAL PREPARATION
I. Step-back technique
- Conventional step-back
- Passive step-back
II. Crown-down (step-down) technique and its modifications
- Crown-down pressureless
- Double flare
- Balanced force
III. Hybrid technique
Passive Step-Back Technique
- This technique was introduced by Torabinejad.
- It involves the insertion of progressively larger hand instruments as deep as they can be passively placed.
- Subsequently, Gates-Glidden drills are used for additional coronal enlargement followed by apical instrumentation using the step-back technique.
WEINE’S MODIFICATION
- For step back technique in curved canals for canal straightening & hour glass preparation.
- Pre-curving of files to minimize canal alteration.
- Removal of flutes from outer curve of the file at apical few millimeters.
- Rasping motion is recommended than reaming.
The three modifications of this technique are as follows:
- Crown-down pressureless technique
- Double-flare technique
- Balanced force technique
Double flare technique:
- FAVA – 1983
Indications: - Straight root canals
- Straight portions of curved canals of mature teeth
Contraindications: - Calcified canals
- Young permanent teeth
- Open apex
Modified double flare technique:
- Advocated by William P Saunder & Elizabeth M Saunder – 1994.
- Uses non-cutting tipped flexible files with balanced force technique.
- Coronal flaring followed by working length determination and apical preparation.
- 40 flex R file with balance force technique introduced in straight part of canal.
- Sequentially larger sizes used to instrument straight part.
- Coronal 4-5mm with GG (2 and 3).
- 20 file extended to WL and canal prepared using balanced force technique.
- MAF varies between 35-40.
- Step back with Balanced force done to prepare remaining curved portion.
Advantages:
- Balanced force helps in less transportation.
- less extrusion periapically.
- less post-op pain.
- Larger apical preparation - easy filling of canal three-dimensionally.
Ultrasonic canal instrumentation
- Suggested by Richman – 1957
- Cavi Endo 1st ultrasonic unit
- These machines transmit low frequency ultrasonic vibration by conversion of electromagnetic energy to the mechanical energy to produce oscillation of file.
- File oscillates at the frequency of 20,000 to 25,000 vibrations/seconds.
- or free movement of file in the canal, it should not have any binding specially at the apical end.
- During the oscillation of file, there is continuous flow of irrigants solutions from the handpiece along the file. This causes formation of cavitation.
- Acoustic streaming is be useful in reducing number of smear layer and loosening the aggregates of the bacteria.
Technique
- Before starting with ultrasonic instrumentation apical third of the canal should be prepared to at least size 15 file.
The root canal debridement depends on:
- Choice of irrigant solution (sodium hypochlorite is irrigant of choice).
- Oscillation of file.
- The form of irrigation with ultrasonic irrigation being supplied.
Advantages of ultrasonic canal preparation
- Less time consuming.
- Produces cleaner canals because of synergetic relation ship between the ultrasound and the sodium hypo chlorite.
- Heat produced by ultrasonic vibration increases the chemical effectiveness of the sodium hypochlorite.
Disadvantages
- Increased frequency of canal transportations.
- Increased chances of overinstrumentation.
CANAL PREPARATION USING SONIC INSTRUMENTS
- Design is similar to ultrasonics.
- They consist of a driver on to which an endosonic file is attached.
- The oscillatory pattern of driver determines the nature of movement of the attached file.
- Sonics cause Cavitation & acoustic streaming; have outstroke shaping motion
- Have longitudinal pattern of the vibration
- This longitudinal file motion produces superior cleaning of the root canal walls.
- Sonic system uses three types of file system for root canal preparation viz. Heliosonic, Rispisonic, Shaper sonic and the canal shaper instruments.
- These files have spiral blades protruding along their length and noncutting tips.
Technique
- After gaining the straight line access to the canal orifices, penetrate small number file in the canal.
- Enlarge the canal up to 20 or 25 number file up to 3 mm of the apex to make some space for sonic file.
- Now insert the sonic file 0.5 to 1 mm short of number 20 file, and do circumferential filling with up and down motion for 30 to 40 seconds.
- After this, use the larger number sonic file and do the coronal flaring.
- After completion with this, determine the working length and prepare the apical third of the canal with hand files.
- Finally blend the apical preparation with coronal flaring using smaller number sonic file.
- Though sonic files have shown to enlarge and debride the canals effectively in lesser time but care should be taken not to force the file apically to prevent instrument separation, ledge formation or canal transportation.
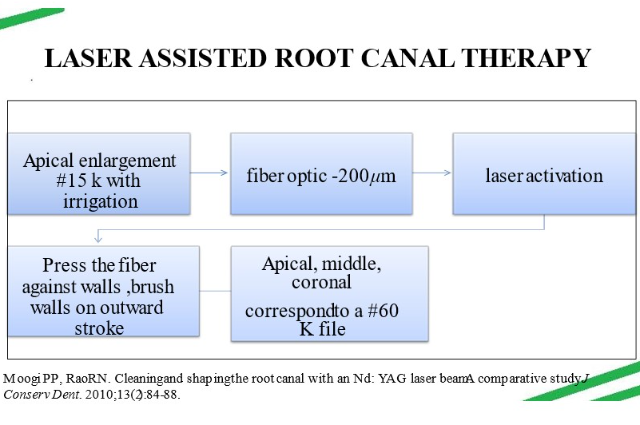
LASER ASSISTED ROOT CANAL THERAPY
- Suggested by Weichman and Johnson in 1971.
- Nd:YAG, Ar, Excimer, Holium, Ebrium laser beam are delivered through the optical fiber with the diameter of 200 to 400 mm equivalent to size 20 to 40 number file.
- Studies have shown different results with lasers.
- Bahcall et al in 1992 found that though the use of Nd:YAG laser can produce cleaner canals, but heat produced by it may damage the surrounding supporting tissues, i.e. bone and PDL.
- Hibst et al showed that use of Er:YAG laser may pose less thermal damage to the tissues because it causes localized heating thereby minimizing the absorption depth.
- Recently a new root canal treatment using the Er, Cr:YSGG (erbium, chromium: Yettruim scandium gallium garnet) has been introduced to help reduce the patient fear and provide better comfort to the patient.
- The device which provides such a treatment is the waterlase—hydrokinetic hard and soft tissue laser, the only laser system to receive FDA clearance for endodontic procedures.
- This laser uses specialized fibers of various diameters and lengths.
- By using hydrokinetic process in which water is energized by the YSGG laser photons to cause molecular excitation and localized microexpansion, hard tissues are removed precisely with no thermal side effects.
- Moreover, antibacterial action of YSGG laser has reduced the use of postoperative antibiotics therapy.
- The intracanal irradiation with laser has shown to reduce the microbial reduction, inflammation, and other postoperative complications.
NON INSTRUMENTATION TECHNIQUE
- Introduced by Lussi and his associates in 1993.
- Technique uses a vaccum pump and an electrically driven piston, generating pressure and bubbles in the irrigation solution, inside the root canal.
- Debris is removed by suction.
- This enhances the ability of NaOCl to dissolve organic pulp tissue.
- The irrigant fluid was injected through the outer tube while the reflux occurred through the inner tube.
Advantages
- Cleaning similar or better than hand instruments.
- Better results in curved canals.
- Less chance of extrusion of irrigant beyond apex.
- Duration independent of the number of canals in tooth.
- This cleanses the canal but, of course, does nothing to shape the canal.
- The hydrodynamic irrigation provoked irritation in the pulpal and/or periapical tissue resulting in bleeding into the root canal.
- Intra-operative problems such as severe pain, underextension and apical extrusion of sealer or breakdown of vacuum have been reported:
Mean % of tissue remnants –coronal(34.4),middle(55.8),apical(76.6) - NIT system is presently not marketed and long-term observations are missing, it can not be regarded as an alternative to mechanical root canal instrumentation.
Technique:
- First reduced pressure at -0.7 bar generated, producing macroscopic and microscopic voids (5-50μm).
- Followed by quick pressure rise to -0.1 bar leading to collapse of bubbles thus building up cavitation and turbulence.
- Allow irrigant to penetrate the whole of the canal system.
- Smooth exchange of irrigant is obtained using double tubing.
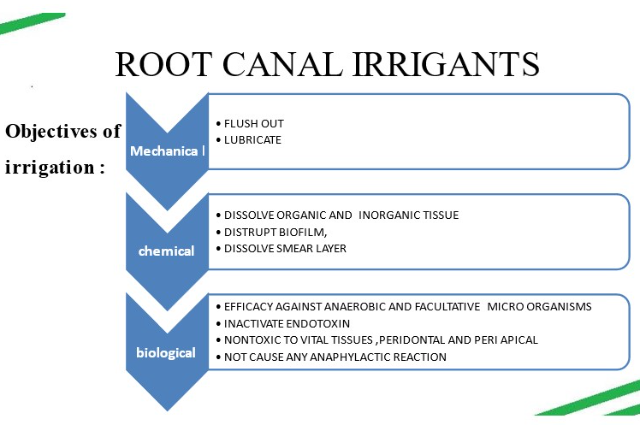
ROOT CANAL IRRIGANTS
- Through the years, different irrigating solutions have been recommended.
- A stream of hot water discharged from an insulated syringe, physiologic saline solution, a 30% solution of urea, urea peroxide solution in glycerine, a solution of chloramine, sodium hypochlorite, and sodium hypochlorite in conjunction with ethylenediaminetetraacetic acid (EDTA) are just a few.
SYRINGES
- Plastic syringes of different sizes (1–20 mL) are most commonly used for irrigation
- All syringes for endodontic irrigation must have a Luer-Lok design. (leak-free connection)
POSITIVE PRESSURE TECHNIQUE P=F/A: - P=PRESSURE DEVELOPED INSIDE THE BARREL
- F=FORCE APPLIED ON PLUNGER
- A=AREA OF PLUNGER
NEEDLES
- In the past, large needles (21–25G) were commonly employed for irrigant delivery.
- Such needles could hardly penetrate beyond the coronal third of the root canal, even in wide root canals.
- More recently, the use of finer diameter needles (28G, 30G or 31G) has been advocated, mainly because they can reach farther into the canal, even to working length (WL).
VAPOUR LOCK
Formation of gas bubbles inside the canal, especially in the apical third, caused by the digestion of organic residues by the NaOCl solution, reducing the penetration of irrigants and so blocking their interaction with the canal walls and inhibiting their antimicrobial and digestive activities.
Syringe irrigation
- Syringe irrigation using 5-mL syringes and fine needles (at least 30G) presents several advantages.
- Closed-ended needles need to be placed at 0–1 mm short of WL.
- Open-ended needles can be placed at 2–3 mm short of WL.
- During irrigation, the needle should be moved longitudinally inside the root canal up to the certain point of maximum insertion.
- Root canals need to be enlarged to size 30 or 35 combined with increased taper, to allow irrigant penetration to WL.
- A relatively high flow rate (~0.25 mL/s) seems to augment both the chemical and the mechanical effects of irrigation.
NAVITIP FX
- Engineered to navigate curved canals without crimping or ledging.
- Available in two gauges and four available lengths allowing delivery of materials of different viscosities directly to the apex.
- Brushed end, for simultaneous delivery of material and scrubing the canal.
- When used with EDTA 18% solution it gently cleans walls of the canals to loosen debris, thus allowing the EDTA to more aggressively “etch” the walls.
- This tip can also be used for scrubbing primers into the canal walls when bonding posts.
- Al-Hadlaq SM et al reported improved cleanliness of the coronal third of instrumented root canal walls irrigated and agitated with the NaviTip FX needle over the brushless type of NaviTip needle.
- 30 gauge needle covered with brush;Better cleaning - coronal third.
- No significant difference in the apical and middle third.
- Friction dislodges brush bristle , difficult to detect even in microscope.
TruNatomy™ Irrigation needle
- Critical to remove bacteria and debris because only 65% of the canal is touched with rotary files.
- Soft, plastic needle can curve and flex with ease, reaching difficult anatomy.
- Two-sided vent for safety
- Atraumatic for hard tissue
ENDO BRUSH
- Nylon bristles set in twisted wire with attached handle.
- Debridemen ~ bristles of the brush ~ extend to the non-instrumented canal walls, fins and isthmus ~ remove trapped tissue and debris.
- Study indicated that instrumentation with the Endobrush was significantly better than instrumentation alone in debriding the root canal.
- However, the Endobrush could not be used to full working length because of its size, which might lead to packing of debris into the apical section.
DISADVANTAGES
- Dentinal tubule disinfection
- Apical terminus penetration
- Biofilm removal
- Isthmus cleaning
ACTIVATION OF IRRIGANTS
- Intracanal Activation Techniques(IAT) improve intracanal cleanliness across a substantial portion of the canal better than conventional needle irrigation (CNI).
- Hence, use of IAT such as Manual dynamic activation (MDA), Passive Ultrasonic Irrigation (PUI), Sonic Irrigation (SI) or Apical Negative Pressure (ANP) are recommended throughout root canal preparation.
ACTIVATION SYSTEMS
- Manual dynamic activation (MDA),
- Sonic irrigation (EndoActivator, Vibringe),
- Continuous ultrasonic irrigation (CUI),
- Passive ultrasonic irrigation (PUI),
- Continuous ultrasonic instrumentation (CUI),
- Self-adjusting file (SAF),
- Photoactivated disinfection (PAD),
- Laser activation (Er: YAG, PIPS).
MANUAL DYNAMIC ACTIVATION TECHNIQUE
- Manual dynamic irrigation can be performed with hand files, brushes, or a well-fitting tapered gutta-percha point.
- It is the apical progression of the instrument that moves the irrigant beyond the tip, and once the working length has been reached, the vertical reciprocating movement used allows the solution to involve the entire canal space.
MODE OF USE
- A well-matching GP master cone whose taper is slightly less than the taper of the canal is selected. A snug fit is sought after at the working length.
- Then 1 ml is trimmed at the tip of the cone in order to get tug-back 1 ml shorter than the canal terminus.
- After suction of the primary irrigant NaOCL, the canal is filled with 1 ml of EDTA delivered with a 30 gauge NiTi needle (either Navy tip from Ultradent or Stropko NiTi Flexi-Tips from SybronEndo or CanalPro Flex-Tips from Coltene/Whaledent)
- Manual agitation of the master cone is started with an up and down motion and a 2 mm amplitude at a frequency of 100 strokes during approximately 1 min.
- After that, 1 ml of EDTA is delivered with the irrigating needle to flush out debris. EDTA is then suctioned to eliminate any residual chelating action.
- The canal is flushed with 1 ml of NaOCl, and the same protocol is repeated using 50 in and out strokes during 30 sec. A final flush is performed with 3 ml of NaOCl.
SONIC ACTIVATION
- Sonic devices range between 1500 Hz and 6000 Hz, and ultrasonic equipment requires vibrations greater than 20,000 Hz.
- Examples:
- EndoActivator® system (Dentsply Tulsa Dental Specialties)
- Vibringe® sonic irrigation system (Vibringe B.V.)
EndoActivator
- Gregorio et al. reported that the EndoActivator® was superior to needle irrigation in getting irrigating solution to the apex of the root canal preparation and into lateral canals.
- However, it was inferior to PUI/UAI and EndoVac® (SybronEndo) for the same role.
Vibringe®
- Rodig et al. reported that use of the Vibringe® resulted in a cleaner apical 1/3 of the canal as compared to needle irrigation alone.
- However, PUI/UAI was superior over the entire length of the root canal.
PASSIVE ULTRASONIC IRRIGATION (PUI)/ ULTRASONICALLY ACTIVATED IRRIGATION (UAI)
- The use of ultrasonic instrumentation in a more passive manner, that is, it was utilized after hand instrumentation and without the intent to enlarge, instrument, or impact the walls of the root canal.
- Thus, the term passive ultrasonic irrigation (PUI) came to be.
- The “passive” portion indicated no active or intentional removal of dentin.
- Research into PUI/UAI has looked at the ability of the technique to remove tissue and debris, bacteria, biofilm, calcium hydroxide and other medicaments, and smear layer.
- After complete instrumentation, passive irrigation for as little as 20 s with NaOCl improved dentinal tubular penetration
- Significantly greater penetration of irrigant into tubules compared to no agitation or alternative agitation methods ( Paragliola et al. 2010)
- Chlorhexidine solutions with or without ultrasonic agitation used, agitation time periods of 1 min and 3 min, revealing that the percentage of killed bacteria depended upon not only the time of exposure, but the chemical formulation of the irrigant as well.
(PUI)/ (UAI) STUDIES
- A large number of studies have reported a significant reduction in the number of bacteria (as measured by colony forming units – CFU’s) following the use of PUI/UAI when compared to needle irrigation.
- Gründling et al. reported that PUI/UAI helped reduce E. faecalis biofilm only when NaOCl was used as an irrigant.
- Malki et al. reported that fluid movement and cleaning extends 3 mm beyond the ultrasonic file tip.
- Malentacca et al. reported no extrusion of irrigant out the root apex when the PUI/UAI file was kept at 3 and 5 mm from the apex.
- However, extrusion did occur when the file was placed within 1 mm of the apex.
- Complete removal of the smear layer after passive US irrigation of NaOCl for 3 min ( Cameron et al. 1893)
- Significant improvement in canal cleanliness after 1 min of ultrasonic activation ( Shen et al. 2010)
CONTINUOUS ULTRASONIC IRRIGATION
- The main disadvantage of PUI is that there is no continuous replenishment of irrigant in the canal and is time consuming.
- Continuous ultrasonic irrigation is achieved by simultaneously and continuously delivering irrigation during ultrasonic activation
- Done through a water port incorporated into ultrasonic tip like ProUltra® PiezoFlow™ or the VPro™ StreamClean™
- The ProUltra® PiezoFlow™ Ultrasonic Irrigation Needle, is a 25-gauge flat open-ended needle made from stainless ssteel that is tightened into the ultrasonic handpiece with a wrench and used in the mid-range power setting in fully instrumented canals.
- The VPro™ Stream Clean Ultrasonic Irrigation System (Vista) is a similar system except that the ultrasonic irrigation needle is a 30-gauge flat open-ended needle that is constructed from nickel–titanium
APICAL NEGATIVE PRESSURE
Negative pressure refers to a situation in which an enclosed volume has lower pressure than its surroundings.
The EndoVac System
The system has three active component parts:
- The Master Delivery Tip (MDT)
- The macrocannula and
- The microcannula.
Master Delivery Tip (MDT)
- The MDT accommodates a syringe of irrigant, which is expressed through a 20-gauge needle.
- There is also a plastic suction hood attached which is connected to clear plastic tubing which inserts into a multiport adaptor which in turn is inserted into the high-volume suction
The macrocannula
- The plastic macrocannula has an external diameter of ISO size of 0.55 mm and an internal diameter of ISO size of 0.35 mm.
- It is made of blue translucent plastic, has a 0.02 taper and is meant for single use only.
The Microcannula
- The microcannula contains 12 microscopic holes and is capable of evacuating debris to full working length.
- These holes act as filters to prevent the clogging of the internal lumen of the microcannula which has an internal diameter of ISO size of 0.20 mm
Evidence-based studies
- Hockett et al. tested the ability of apical negative- pressure irrigation to remove a thick biofilm of E. faecalis in mesial roots of mandibular molars, finding that these specimens rendered negative cultures after 48-h incubation, while some of those irrigated using traditional positive-pressure irrigation were positive at 48 h.
- One in vivo dog study found that apical negative pressure irrigation with 2.5 % NaOCl resulted in similar bacterial reduction than the use of apical positive-pressure irrigation combined with seven days of intra-canal medication which was the triple antibiotic paste.
CONTINUOUS INSTRUMENTATION AND IRRIGATION; THE SELF-ADJUSTING FILE (SAF) SYSTEM
- The effective cleaning of oval canals is a challenge that is beyond the ability of syringe and needle irrigation.
- The action of rotary files in such canals not only fails to clean the buccal and/or lingual “fins” or the isthmus between canals but also actively packs these recesses with dentin particles that are difficult to remove, even with passive ultrasonic irrigation.
- It is based on using a hollow file that adapts itself to the shape of the canal, rather than the common concept of shaping every canal to a round cross-section.
- It removes a uniform layer of dentin all around the perimeter of the root canal; thus, a round canal is enlarged to a larger round canal, but a flat-oval canal is prepared to a flat-oval shape of larger dimensions.
- The hollow file allows continuous irrigation through its lumen; thus, irrigation occurs continuously and simultaneously with instrumentation.
The self-adjusting file (SAF)
- The SAF is the first file that does not have a solid metal core.
- The file is designed as a hollow tube, in which the walls are made from a thin nickel titanium lattice with a rough outer surface. The tube has an asymmetrically positioned tip.
- The file is extremely compressible, such that a 1.5 mm SAF diameter may be compressed into a root canal that only a #20 K file can be inserted into.
The RDT handpiece head
- The RDT handpiece head has a dual mechanical function.
- It transforms the rotation of the micromotor into a trans-line in-and-out vibration with an amplitude of 0.4 mm and contains a clutch mechanism that allows the SAF to rotate slowly when not engaged in the canal but that completely stops the rotation once the file is engaged with the canal walls.
Endostation/VATEA irrigation pumps
The SAF is provided with a freely rotating hub to which a polyethylene tube is connected, thus allowing the irrigant to flow through the hollow file into the root canal.
No-pressure irrigation
The SAF may be defined as a no-pressure irrigation system that is applied throughout the instrumentation process.
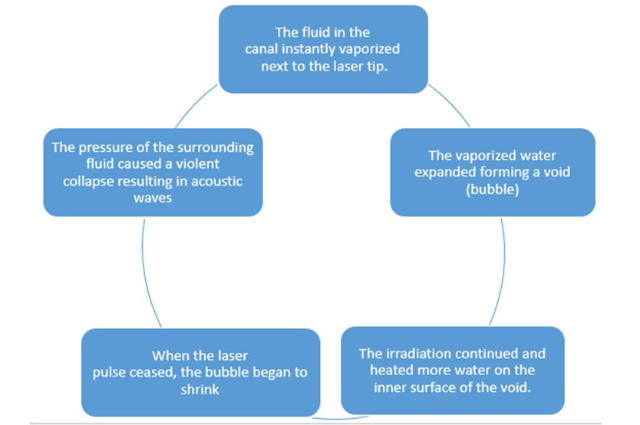
LASER-ACTIVATED IRRIGATION (LAI)
- Bactericidal action of the laser depends on the wavelength and energy, and in many cases it is due to thermal effects that produce alteration of the cell wall of the bacteria, leading to changes in osmotic gradients up to cell death.
- The mechanism of this interaction has been attributed to the effective absorption of laser light by sodium hypochlorite.
- This leads to the vaporization of the irrigant and to formation of vapor bubbles, which expand and implode with secondary cavitation effects.
IRRIGATION OF THE ROOT CANAL SYSTEM BY LASER ACTIVATION (LAI): PIPS PHOTON-INDUCED PHOTOACOUSTIC STREAMING
- PIPS is a form of laser-activated irrigation that works indirectly and without thermal effects by activating irrigants.
- Its mechanism of action is by creating a strong photoacoustic shockwave that streams irrigants three dimensionally throughout the root canal system.
- This creates an expansion and successive shock waves leading to the formation of a very powerful streaming of the fluid located inside the root canal, with no rising of temperature.
PIPS Protocol
- The PIPS tip is placed in the pulp chamber only (not in the root canal) and held stationary throughout the activation process.
- During the time of laser(Er: YAG laser) activation, the dental assistant applies a continuous flow of the solution from the dental irrigating syringe.
- The laser activation period for PIPS is in 30 s cycles.
- The current protocol is six 30 s cycle of laser activation.
PHOTODYNAMIC THERAPY FOR ROOT CANAL DISINFECTION
- Antimicrobial photodynamic therapy works as a combination of photosensitizer and light.
- Photosensitizer is a light-sensitive chemical that possesses low toxicity in the absence of light.
- Photosensitization of the infected tissue with a photosensitizer allows uptake into the bacterial cells, and irradiation of the photosensitized tissue with a specific wavelength laser results in the destruction of bacteria and infected tissue.
- The commonly used photosensitizers for antibacterial purpose are:
a. Halogenated xanthenes such as rose bengal (RB),
b. Phenothiazines such as methylene blue (MB) and
c. Toluidine blue (TBO), and
d. Perylenequinones such as hypericin
GENTLE WAVE SYSTEM
- Multisonic technology – multiple acoustic frequencies at same time.
- Technology is paired with optimized procedure fluids.
- Broad spectrum acoustic energy.
CONCLUSION
- Shaping and cleaning are important interdependent steps in the root canal treatment.
- The combination of anatomic, biologic & pathophysiologic knowledge of the tooth, various instrumentation techniques, & the skill of the operator play a major role in optimizing the quality of root canal treatment.
. . .
References:
- COHEN’S PATHWAYS OF PULP
- ENDODONTIC IRRIGATION SPRINGLER
- TEXTBOOK OF ENDODONTICS GROSSMEN
- Review of Contemporary Irrigant Agitation Techniques and Devices. Li-sha Gu et al. JOE — Volume 35, Number 6, June 2009
- Modern Endodontic Principles Part 4: Irrigation.Darcey J, Jawad S, Taylor C, Roudsari RV, Hunter M.Dent Update. 2016 Jan-Feb;43
- Ultrasonics in Endodontics: A Review of the Literature: Gianluca Plotino, JOE 2007
- Paqué F, Laib A, Gautschi H, Zehnder M. Hardtissue debris accumulation analysis by high resolution computed tomography scans. J Endod. 2009;35:1044–7.
- De-Deus G, Souza EM, Barino B, Maia J, Zamolyi RQ, Reis C, Kfir A. The self-adjusting file optimizes debridement quality in oval-shaped root canals. J Endod. 2011;37:701–5.